When we think about evidence-based practice, we consider the level of evidence supporting what we plan to implement. There are levels of evidence quality to consider.
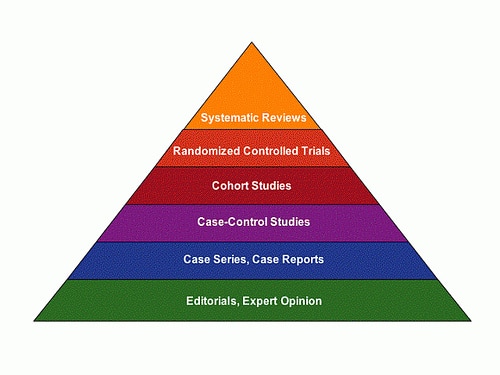
Editorial or expert opinion: What you think sounds good, what your grad school professor suggested, etc. No matter how good the idea might sound, the evidence level of expert opinion is extremely low. Oral motor treatments are backed by this level of evidence (however, in randomized controlled trials, oral motor treatments were shown not to work). PROMPT is also backed by this level of evidence. Although PROMPT has been studied in two case reports, they were not peer reviewed, so the level of evidence remains at an editorial level. If I tell you that playing with pink trains makes my kiddos speak better, the level of evidence is the same as PROMPT or oral motor. People can say anything they like. The wisest thing is not to run with their opinion until they back it up with a higher level of evidence, especially if there is a treatment backed by a higher level of evidence.
When we see that one treatment is backed by a description of how a single child or a few children did, the study is called a case report or case series. The evidence level is rather low. When the disorder is less common, such as certain syndromes, case studies may be all that is possible. However, if the disorder is more common, such as speech sound disorders, and the only evidence presented is a case report, clinicians should be cautious about using the treatment.
Case-control studies refer to looking at a group based on a factor you are interested in (such as children who have stubbed their toe) and comparing them to a group who do not have the factor you are interested in. Obviously there are participant selection issues here, which is why this kind of study is not up with RCTs. The traditional, developmental articulation approach is backed by this level of evidence but not for severely-profoundly unintelligible children.
A cohort study is similar to a case-control study in that there are two groups, but in a cohort study the groups are selected beforehand. Let's say you wanted to know if a treatment worked; to conduct a cohort study, you would select the groups before initiating treatment.
Randomized controlled trials are considered a high level of evidence, because not only are there two groups and a comparison between groups, the participants in each group were randomly selected. This is the highest level of evidence we typically have as far as study design (because double blinding is typically not possible in our field).
Systematic reviews, also known as meta-analyses, are overviews of peer-reviewed, published studies. They are the highest level of evidence in our field. Cycles is backed by this level of evidence, as is metaphonological skills training.
When we see that one treatment is backed by a description of how a single child or a few children did, the study is called a case report or case series. The evidence level is rather low. When the disorder is less common, such as certain syndromes, case studies may be all that is possible. However, if the disorder is more common, such as speech sound disorders, and the only evidence presented is a case report, clinicians should be cautious about using the treatment.
Case-control studies refer to looking at a group based on a factor you are interested in (such as children who have stubbed their toe) and comparing them to a group who do not have the factor you are interested in. Obviously there are participant selection issues here, which is why this kind of study is not up with RCTs. The traditional, developmental articulation approach is backed by this level of evidence but not for severely-profoundly unintelligible children.
A cohort study is similar to a case-control study in that there are two groups, but in a cohort study the groups are selected beforehand. Let's say you wanted to know if a treatment worked; to conduct a cohort study, you would select the groups before initiating treatment.
Randomized controlled trials are considered a high level of evidence, because not only are there two groups and a comparison between groups, the participants in each group were randomly selected. This is the highest level of evidence we typically have as far as study design (because double blinding is typically not possible in our field).
Systematic reviews, also known as meta-analyses, are overviews of peer-reviewed, published studies. They are the highest level of evidence in our field. Cycles is backed by this level of evidence, as is metaphonological skills training.